



In this article I want to try to explain to you in the simplest way possible, those that are the most frequent shoulder injuries in the CrossFit® population.
We will go to analyze what they are caused by these injuries, starting from joint physiology and anatomy (explained in super simple words), and then go on to analyze what we can do to solve this problem.
Since I will have a lot to say, let's start right away!
Index
ARCHITECTURE AND SHOULDER FUNCTION


Before addressing and discussing what potential shoulder injuries are, it is worth discussing of its architecture and its function.
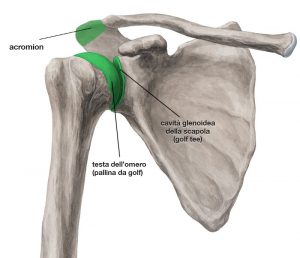
The shoulder joint, called glenohumeral joint, we can imagine it as one "golf ball"Resting on his"tee"(That plastic contraption where the ball rests).
If you are a golfer you will probably notice one thing right away; if you are not, I'll explain it to you: the golf ball (which in our simile is the head of the humerus) it is extremely larger than its tee (glenoid cavity of the scapula).

In fact, Mother Nature wanted the shoulder to be the most mobile joint in our body, at the expense of its stability.
In order to overcome this problem, he has thus created structures that, in some way, increase this stability; such as the glenoid labrum, the rotator cuff, and the various ligaments.
For this reason, we can understand how this instability is often the cause of shoulder injuries.
THE SHOULDER JOINTS
However, there is also another clarification to make: when we talk about the shoulder joint, we should actually refer to a much larger joint complex.
In fact, not only the head of the humerus and the glenoid cavity of the scapula are part of this joint, but there are also other joints such as the sternoclavicular, acromion-clavicle, scapulo-thoracic, etc ...
All of these joints work in synergy to ensure correct shoulder movements.
You can therefore immediately understand how it is enough for just one of these joints to work badly to compromise the normal harmony of movement of the shoulder, leading it to a possible accident.
SHOULDER INJURIES
Shoulder injuries generally fall into three broad categories:
- Injuries due to incorrect technique in sports gestures
- Injuries related to shoulder instability
- Accidents related to an imbalance between the primary motors and the stabilizers
However, in clinical practice and especially in the world of athletes, the most frequent shoulder injury is that caused by an imbalance between the primary motors and the stabilizing muscles.
So in this article we will go to deepen just this topic.
To understand the mechanics of injury we must start from what is the normal joint physiology
JOINT PHYSIOLOGY
As we have said, the various shoulder joints must work in synergy to ensure optimal arm movements; that is shoulder flexion-extensions, abductions and adductions, and intra and extra rotations.
Earlier we mentioned the scapulo-thoracic joint, and this is often the defendant in the shoulder injury.
At the shoulder level it exists a pseudo-joint which is what happens between the shoulder blade and the chest; physiologically it should happen that when we raise, for example, the arm, the scapula rotates externally following its movement.
This is called the scapulohumeral rhythm, and serves to prevent the head of the humerus from bumping into the acromion, a small bony protrusion of the shoulder blade, where in the middle (between the head of the humerus and the acromion) it passes a muscle of the rotator cuff: the supraspinatus muscle.
So it results that if this scapulo-humeral rhythm is altered, and therefore it is not optimal and physiological, the head of the humerus can impact against the acromion, causing the phenomenon that is known as subacromial impingement, which is nothing more than an "entanglement" of the supraspinatus muscle which remains entangled between the head of the humerus and the acromion.

To avoid this condition, therefore, it is necessary that the scapulohumeral rhythm is physiological. Therefore, when we move the arm, the scapula should always follow the movement, turning its glenoid cavity upwards, so as not to impact the head of the humerus on the acromion.
Sometimes, due to an imbalance between the primary motor muscles such as the deltoid and the stabilizing muscles such as the rotator cuff, the serratus anterior and the rhomboids, this does not happen; in fact there is often an imbalance between these muscles and, in particular, there is frequently a weakness of the anterior serratus and of the cuff muscles.

The serratus anterior has the task of stabilizing the scapula on the thorax thus ensuring correct movement, and in the same way the rotator cuff must be strong enough to keep the head of the humerus centered within the glenoid cavity.
If these two muscle groups are too weak compared to the deltoid muscle, which is a very strong muscle, it happens that when this (the deltoid) is activated, due to its normal physiology, it pulls the head of the humerus upwards.
If this is not counteracted by the stabilization of the rotator cuff and the serratus anterior, it causes what we have just called subacromial impingement.
SUMMING UP…

We can outline the causes of subacromial impingement, that is the conflict between the humerus and the acromion, as an altered scapulohumeral rhythm, and therefore not physiological, resulting from a weakness of the stabilizing muscles, especially of the anterior dentate and rotator cuff muscles.
"Okay, I have shoulder pain, but how can I tell if this is my problem?"
Well, the first thing you can do, quite simply, is a visual evaluation; therefore, you can film yourself, back to back, with your phone as you try to raise both arms at the same time.
Under normal conditions you should notice that the two shoulder blades move roughly at the same time.
If, on the other hand, while you raise your arms you notice that one shoulder blade anticipates the movement or delays the movement compared to the other, or when you lower them it delays its return to its normal position, you may have this problem.
But to evaluate this issue, the advice is always the same: contact a professional who will be able to give you the correct information.
HOW TO MANAGE SHOULDER PAIN CONDITIONS
What I will tell you now is absolutely effective for the problem we have described above and is equally effective for the prevention of shoulder injuries.
So no matter what problem you may have, you can definitely benefit from these tips.
What we need to do, in a nutshell, are mainly three things:
- Strengthen the stabilizing muscles of the shoulder
- Restore a correct scapulohumeral rhythm
- Strengthen the depressor muscles of the humerus
REINFORCEMENT AND RESTORATION OF MOVEMENT
The rotator cuff brace is definitely one part fundamental to be included in your recovery program, and then to be maintained in a preventive perspective.
Generally the cuff is reinforced and trained through theuse of rubber bands, but there are numerous exercises, even free body, or with the use of other tools, that you can do to improve its effectiveness.
To restore a correct rhythm of the scapula on the chest instead, it is necessary to go to train those muscles that keep it attached to the rib cage itself.
One above all is the anterior serratus muscle, which we can go to train, for example, through scapula push-up; an exercise as simple as it is effective.
Another exercise that I personally consider very valid is it scapula pull-up, which trains the entire shoulder girdle, including the depressor muscles of the humerus, or those muscles that somehow counteract the forces caused by the deltoid in elevation.
In fact, in addition to the muscles that stabilize the joint, it is also essential to train those who are the antagonists of a certain movement.
If we have to counteract the movement of elevation of the humerus, we do it by training and strengthening the great dorsal muscle, which is instead a depressor and extensor of the humerus.
IN CONCLUSION
We have seen a very general overview of what are the injuries and problems related to the shoulder, and how we can go about solving them.
I hope, as always, to have been as clear and simple as possible in explaining the topic, which is not always a foregone conclusion, as it is difficult to summarize everything in a simple article on such complex topics.
My advice remains to consult other guides, other videos, but above all to consult a specialist! Greetings and see you next time!


He practiced Rugby since the age of 7, serving in the ranks of the Serie A with the team of his city, Alghero, while currently, he is dedicated to CrossFit for about 3 years and under study.
Big passionate about Scientific Literature and Physiotherapy, and its mission is to try to spread it to as many people as possible, so that they become more aware!
Instagram Profile: @robertobombagi_, Page: @fisiomagazineit,
website: www.fisiomagazine.com